Commercial Payers → Implementation → Retention for Commercial Plans and Employers
Retention for Commercial Plans and Employers
Retaining plan members who have elected to participate in the National DPP lifestyle change program is an important program objective. The longer an individual stays in the program, the better his or her outcomes. Retention also impacts the ability of a CDC-recognized organization to maintain CDC recognition and receive performance-based payments.
This page contains the following topics:
- Retention Improves Outcomes
- Retention Best Practices
- Retention Strategies in Practice
- Tailoring Retention Practices in Rural Areas
- Using Incentives
- Incentives in Practice
- Retention Statistics
Retention Improves Outcomes
Research from CDC’s Diabetes Prevention Recognition Program (DPRP) 2017 dataset has shown the longer a person stays in the program, the better their outcomes. For example, CDC has found that there is a significant association between staying in the program past the first 16 weekly sessions and achieving the 5%+ weight loss. Participants that remain in the program for 17+ sessions (the second six months of the program) achieve weight loss at higher rates than those in the program for the first 16 sessions (the first six months of the program).
Additional retention and outcomes statistics from CDC analyses on the DPRP 2017 dataset are indicated below.
- Analyses on three weight loss distributions (low, medium, and high weight loss) found that individuals in all three groups, regardless of amount of weight loss, exhibited the same trend: those attending 17+ sessions and having an average of 150+ minutes of physical activity per week had increasingly higher percent weight loss among all race/ethnicity groups.
- For women with gestational diabetes mellitus, significant predictors of achieving 5% weight loss were meeting the 150 minutes of physical activity, attending ≥ 17 sessions, staying in the program for more than 183 days, and age 45–64 years.
- For every additional session attended and every 30 minutes of activity reported, participants lost 0.3% of body weight (p < 0.0001). See the ADA report here.
Health-Related Social Needs (HRSN) Impact Retention
Efforts to improve retention in the National DPP lifestyle change program often require broader approaches that address social, economic, and environmental factors that influence health. Social determinants of health (SDOH), are conditions in the environments in which people are born, live, learn, work, play, pray, and age that affect a wide range of health, functioning, and quality of life outcomes. While everyone has socially determined factors of health, some populations and individuals may have health-related social needs (HRSN) stemming from these factors. While SDOH are broader social conditions, HRSN are more immediate individual or family needs impacted by those conditions. They include housing insecurity, food insecurity, or lack of reliable transportation that can lead to decreased health and a lower quality of life.
HRSN may serve as a barrier to both access and continued participation in the National DPP lifestyle change program. An increasing number of CDC-recognized organizations are structuring their programs so that some of these barriers to participation can be overcome, such as allowing for the provision of childcare vouchers and access to healthy food. For examples of how a CDC-recognized organization can address HRSN, see Addressing HRSN Through the National DPP Lifestyle Change Program page of the Coverage Toolkit.
For more information on SDOH and HRSN as they relate to the National DPP lifestyle change program, visit the suite of Health Equity and the National DPP pages on the Coverage Toolkit.
Retention Best Practices
Best Practices Guide
NACDD, Leavitt Partners, and the Minnesota Department of Health partnered to compile evidence- and experience-based best practices on recruitment, enrollment, and retention into a single Best Practices Guide. The guide is written for lifestyle coaches and program coordinators who serve low income, Medicaid-eligible participants. However, many of the principles discussed in the guide could be used by commercial plans and employers working to increase recruitment, enrollment, and retention in the National DPP lifestyle change program and would apply to all eligible program participants.
The Best Practices Guide contains nine retention related best practices. For each best practice, the guide includes the rationale behind the practice, tips for action, linked resources, and implementation examples from lifestyle coaches and program coordinators. In conjunction with the guide, the Minnesota Department of Health released a series of videos interviewing lifestyle coaches and program coordinators to emphasize the retention strategies detailed in the Best Practices Guide. The videos are linked in the best practices below.
Below is a short description of each best practice and how it could be applied in a commercial plan or employer setting. Employers and commercial health plans must comply with all health information privacy laws when implementing the National DPP lifestyle change program and interacting with employees or members in relation to the program.
1. Meet Unique Participant Needs
Enhance the National DPP lifestyle change program to meet the needs of specific participants. Enhancements may be tailored around the participants’ cultural community, gender, age, literacy level, disabilities, income level, and location (e.g., rural vs. urban). For example, address SDOH through the use of community health workers (CHWs) for culturally appropriate program delivery and utilize culturally relevant food and menu examples. Pages 27-29 of the Best Practices Guide provide a list of publications describing considerations and enhancements for various populations.
2. Use Low-Literacy Materials
Incorporate the use of additional low-literacy materials, such as visuals and materials written at a 6th grade level or below, to address SDOH-related educational barriers. If needed, provide support in using a digital device for those participating in the program online or through distance learning.
3. Address Barriers to Participation
Find creative solutions to address the common barriers that prevent participants from enrolling and/or continuing in the program, including SDOH-related barriers, such as addressing childcare or transportation concerns, and making it easier for participants to catch up on missed sessions.
4. Expand Flexibility through In-Person, Online, and/or Distance Learning Program Delivery
Increase access to the National DPP lifestyle change program by offering a combination of in-person, online, and/or distance learning delivery of the program. Access can also be increased by offering the program at or close to the worksite, and at various times of day.
5. Encourage Social Connections
As appropriate, facilitate social connections between program participants during and outside of sessions such as through setting up a private social media group for the participants and organizing physical activities. Employers should be particularly mindful of addressing any potential group dynamic issues, including privacy concerns.
6. Offer Supplementary Experiences
Add variety and interest by offering unique supplementary experiences to participants, such as a grocery store tour, cooking demonstrations, or guest speakers.
7. Tailor Communications to Participants
As appropriate, contact program participants to encourage continued participation, and tailor the mode of communication to the preferences of the participants.
8. Use Incentives
Provide incentives related to healthy living. Additional information about incentives that is complimentary to what is found in the Best Practices Guide can be found in the Using Incentives section below.
9. Provide Lifestyle Coach Training
Improve the participants’ experience by using a team of highly skilled lifestyle coaches that participate in continuing lifestyle coach education.
CDC Retention Resources
Retention Tip Sheet
CDC has developed a tip sheet that provides insights and lessons learned about improving participant retention, including how to establish participant buy-in, retention strategies for months 7-12, and how to build the capacity of lifestyle coaches to increase retention.
Personal Success Tool
CDC created the Personal Success Tool (PST) to help increase participant retention. It has interactive, web-based modules to encourage participants, reinforce information they have learned in class, and provide tailored support to meet their needs. The PST is based on behavior change theory and audience research, and has been tested by coaches and participants in nine National DPP lifestyle change programs. It includes motivational messages, testimonials, short games, quizzes, and participant pledges.
Who uses the PST?
The PST is designed for lifestyle coaches and National DPP lifestyle change program participants. Coaches use the PST to help participants stay engaged by sending related modules after each class. Participants can review the modules on a computer, smartphone, or tablet, and each activity only takes a few minutes to complete.
The PST is designed to follow the order of the PreventT2 curriculum, but can be used with any CDC-recognized National DPP lifestyle change program curriculum.
Lifestyle Coach Perspectives on the PST
- “Using the Personal Success Tool will help you stay motivated when you need extra encouragement.”
- “Completing the modules will reinforce what you learn in class, helping you master new ideas, and continue to be successful in the long term.”
- “…the PST is easy to use and only takes a few minutes to review during class.”
PST Resources for Lifestyle Coaches
- Lifestyle Coach’s Guide—an overview of the PST, including when and how to use it
- Quick Reference Guide—a printable worksheet to schedule when to send each module to program participants
- PST Talking Points—ideas on how to introduce the PST to program participants
- PST Participant Overview—a handout for program participants about the PST
Retention Strategies in Practice
The tabs below describe how various organizations have put retention strategies into practice.
Commercial Health Plan
One commercial health plan has delivered over 40 classes and has supported over 450 individuals in participating in the National DPP lifestyle change program. It delivers most of its sessions at community wellness centers, several of which are co-located with physician offices. These centers are located in communities with high prevalence of diabetes and obesity and significant disparities in care. The retail centers tend to be highly accessible to individuals in the surrounding area.
The health plan’s National DPP program manager cited the following as success factors in retaining participants in the National DPP lifestyle change program:
- Staffing the program with individuals who are able to connect to the communities, such as coaches who are reflective of the populations they are serving
- Having social workers on-location where the classes are held to help with additional needs that affect the individuals’ ability to adhere to the program
- Upholding a strong relationship with the primary care physicians
Solera Health
Solera Health, a preventive care benefits manager, contracts with employers and health plans that cover the National DPP lifestyle change program. The following practices have been critical to Solera for retention of participants:
- Allowing participants to easily choose or be matched to the CDC-recognized organization that best meets their needs
- Personalizing program messaging and delivery
- Allowing participants to make up missed sessions using online technology
- Ensuring there are frequent interactions between the lifestyle coach and the program participants
- Offering a wearable fitness tracker as an incentive for completion of the fourth session
YMCA
A senior director of evidence-based health interventions at the YMCA of the USA indicated that the following factors contributed to retaining participants:
- Ensuring that lifestyle coaches had strong facilitation skills, empathy, and can support an effective group dynamic
- Educating participants about the requirements of the program prior to the first session (including the program’s duration and the likely challenges of achieving behavior change)
Tailoring Retention Practices in Rural Areas
Various studies on diabetes education and prevention programs in rural areas have indicated the following factors as contributing to successful implementation:
- Providing participant transportation to classes when needed
- Hosting the program in a common, well-known location
- Developing positive relationships with and engaging providers, social workers, and other community stakeholders
- Considering cultural sensitivities and differences between counties when recruiting and engaging participants
- Establishing support from community leaders
- Educating communities on the underlying SDOH factors
- Helping communities better understand their capacity, assets, and resources
- Gaining an understanding of local politics
- Offering the program via telehealth to increase access
The studies summarized above are found here: Appalachia, Montana, Montana telehealth, Federal Office of Rural Health Policy (FORHP).
In addition, NACDD collected the following information from state and local health department representatives from Montana, Colorado, North Dakota, and Ohio regarding challenges facing rural populations and opportunities to mitigate those challenges.
Access

- Lack of lifestyle coaches or CDC- recognized organizations
- Limited broadband internet access in some rural areas
- Online delivery options, where internet is available
- Program delivery in-person and via telehealth technology to remote sites (for an example of how telehealth delivery can be implemented, see the Montana State Story of Medicaid Coverage page of the Coverage Toolkit)
- Encouraging the following to deliver the program: Cooperative Extension System through land grant universities; places where people already gather such as community and senior centers, churches, and libraries; and hospital systems that have identified obesity as a priority through community health assessments
Travel Time
- Travel distances—both for coaches and participants—can be further in rural areas
- Encouraging carpooling, which also enhances opportunities for support
- Use “buy one, get one free” registration deals to engage spouses or friends
- Providing gas cards as incentives
- Have several lifestyle coaches trained in each organization to share the travel burden
Participants Moving

- Participants may move to a different location throughout the year
- Allow participants to join a class at other locations so they can complete the yearlong program
Participation

- A less populous area can make it difficult to enroll enough participants
- Word of mouth is very powerful in rural areas
- Use “buy one, get one free” registration deals to engage spouses or friends
- Delivery organizations developing a collaborative service delivery model to increase class options for participants and increase enrollment for all sites
Marketing

- Finding a marketing strategy for the rural population
- Local radio
- Local free newspapers available in grocery stores
Lifestyle Coach Support

- Since lifestyle coaches may be spread out, it may be difficult to support them
- Monthly support calls and annual face-to-face meetings to offer refresher training, support, resources, and best practices
Recruitment and Referrals
- Because of the diffused population, it may be difficult to identify potential participants
- Support from rural health/hospital systems is critical as it may be the only medical care in the area
- Screening and testing through employers is also key
- Having a neutral party organize referrals (e.g., the Cooperative Extension) allows providers to have one number for referrals to programs
- Gaining buy-in from local health care providers and hospitals
Using Incentives
Some CDC-recognized organizations and their partners use incentives to enhance participant enrollment and retention. Incentives can also ease the burden of SDOH-related economic instability and allow participants to remain in the National DPP lifestyle change program. In general, programs have shown to have higher attendance rates when they include incentives.
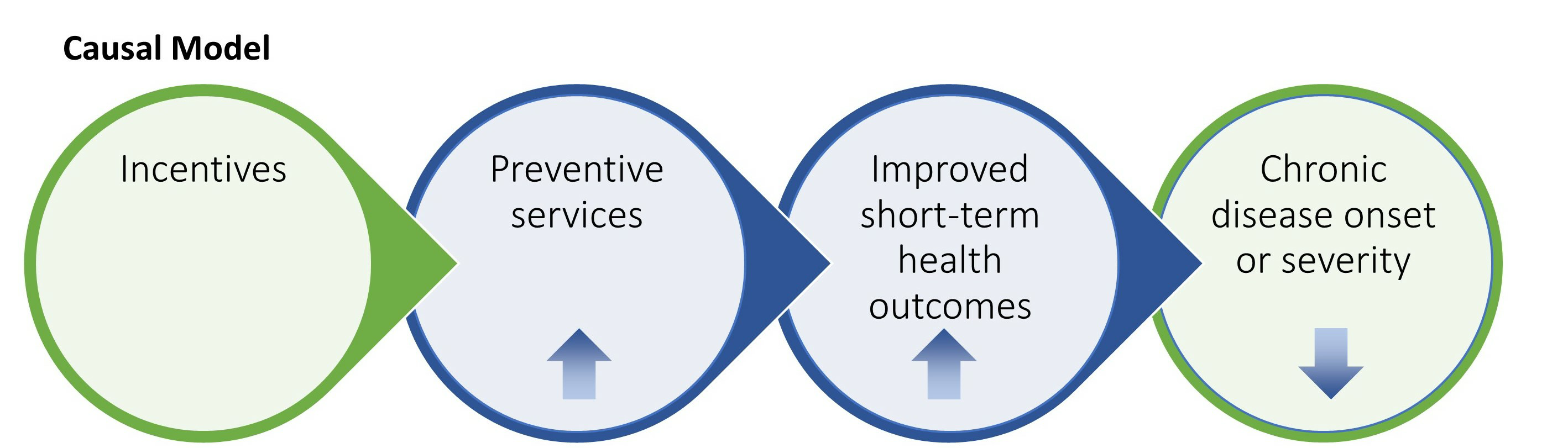
Source: MIPCD Final Evaluation Report – Figure E-2
There are many characteristics of a good incentive program that are important to consider. It will be important to determine:
- Who will receive the incentive
- What type of incentive will be given (e.g., cash, vouchers, gifts, etc.)
- What target or goals will need to be achieved to receive the incentive
- When participants will receive the incentive (e.g., immediately following achievement of the target or goal, on a fixed schedule, etc.)
- What the value of the incentive will be
- Whether the incentive is guaranteed (e.g., when using a lottery method, the incentive is not guaranteed)
- Whether the incentive employs a positive (carrot) approach for engaging in a healthy behavior or a negative (stick) approach where a loss is achieved for not engaging in a healthy behavior or achieving an outcome.
- Whether the incentive is aligned with program goals and provides additional support for individuals to achieve the desired outcomes

The sessions during the last six months of the program emphasize maintaining a healthy lifestyle that was learned in the first six months of classes. Participation in these classes provide continued support and motivation to the program individuals seeking to retain a healthy lifestyle. When developing incentives, steps should be taken to develop a model that encourages participants to maintain participation throughout the second six months of the program, in addition to the first six months.
Incentives in Practice
The examples below describe how various organizations have approached offering incentives in their National DPP lifestyle change programs.
Commercial Health Plan
One commercial health plan, for instance, observed that participation and retention is stronger among groups that offer incentives, so has encouraged employers to provide incentives based on completing 16 sessions. The health plan’s initial incentive plan offered “points” for completing the 4th, 9th, and 16th sessions, which could then be used to “purchase” non-monetary incentive items. However, after evaluating the incentives and participation, and finding that many participants would discontinue after the 9th session, the incentive program was changed to favor completion of the 16th session. As a result of the change, retention through the 16th session increased. The health plan found that non-monetary incentives, such as awarding wearable fitness trackers after program completion, were also successful.
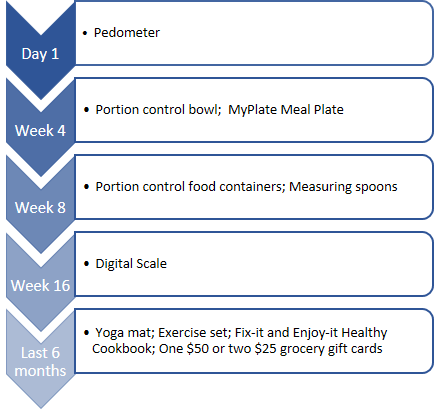
Maryland
One Maryland MCO that participated in the Medicaid Coverage for the National DPP Demonstration Project provided various incentives according to the schedule below.
To learn more about how the Medicaid Coverage for the National DPP Demonstration Project was implemented in Maryland and Maryland’s plan for ongoing sustainability of the program, visit the Maryland Medicaid Demonstration Project page of the Coverage Toolkit.
Minority Diabetes Prevention Program
North Carolina received state funds through their Office of Minority Health and Health Disparities to establish North Carolina’s Minority Diabetes Prevention Program, which focuses on increasing minority access to and participation in National DPP lifestyle change programs. It provided grant funding to partners across the state to market and administer the program. Some of the partners used incentives to promote healthy habits according to the schedule below. 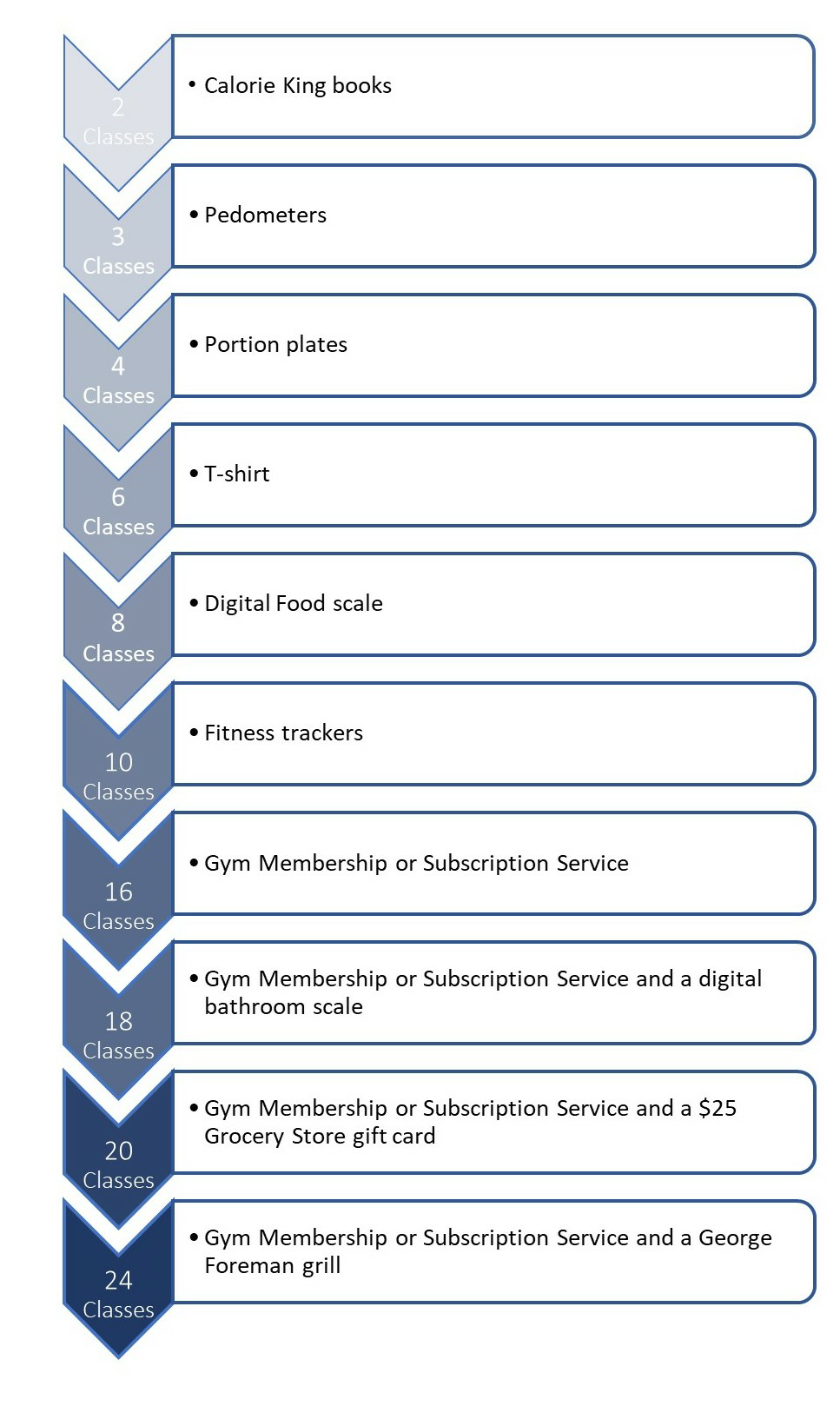
Six National Organizations
In 2012, CDC funded six national organizations through a five-year cooperative agreement to scale and sustain multistate networks of CDC-recognized organizations to deliver the National DPP lifestyle change program. A study based on this effort found that most of the CDC-recognized organizations offered the following three types of incentives to retain participants in the National DPP lifestyle change program. The incentives were program-funded and were not supported by federal funding.
- Non-monetary Incentives
- Incentives included gym memberships, pedometers, food-measuring devices, or cookbooks
- Used by 118 of the reporting CDC-recognized organizations (78.7%)
- Monetary Incentives
- Incentives included coupons or gift cards (less than $25 value)
- Used by 32 of the reporting CDC-recognized organizations (21.3%)
- Removal of Barriers of Access
- Incentives included childcare or transportation passes
- Used by 29 of the reporting CDC-recognized organizations (19.3%)
Only the non-monetary incentives were found to significantly impact attendance. When non-monetary incentives were used participants attended an average of 1.8 more sessions and participated in the program an average of 27.8 more days.
Another retention tool utilized by the CDC-recognized organizations was cultural adaptation (e.g., using cultural images, and incorporating cultural dietary restrictions and preferences). When cultural adaption was used participants attended an average of 1.4 more sessions and participated in the program an average of 29.5 more days.
State Employee Plans
One state employee plan offered the National DPP lifestyle change program as part of a wellness benefit. It would offer participants points after completing each class, which accumulated throughout the program. The plan had a wellness platform through which participants could use their points to “purchase” health- and fitness-related items.
Another state employee plan found that when outreach mentioned the incorporation of incentives, enrollment was roughly 10 times greater than when outreach did not mention incentives.
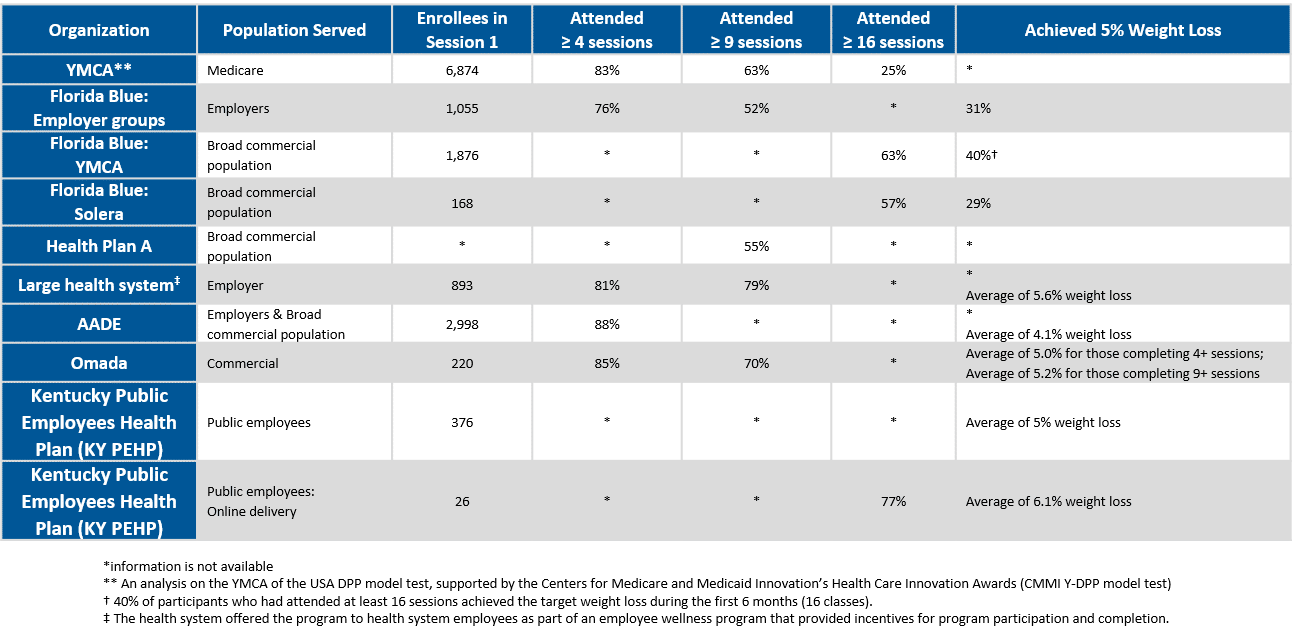
Retention Statistics
The table below shows retention statistics from various health insurance plans, employers, and CDC-recognized organizations who have implemented the National DPP lifestyle change program. More detailed summaries on a few of these programs can be accessed in the Florida Blue case study, the Association of Diabetes Care and Education Specialists (ADCES) (formerly American Association of Diabetes Educators (AADE)) infographic, and the YMCA of the USA DPP 2015 Annual Report (published in March 2016). The YMCA report is from an implementation of the National DPP lifestyle change program with Medicare beneficiaries that was supported by the Centers for Medicare and Medicaid Innovation’s Health Care Innovation Awards. For additional data reports from this project, see CMS’ Health Care Innovation Awards page.